Stripped of hype, trends and outdated slogans, and aligned with where cardiometabolic science and cholesterol has currently landed.
Let’s face it, for most people the only time you come across the terms LDL and HDL are probably when you have your blood works done at your Dr’s and even then, tucked in with the rest of your lipid profiles they may just say, your cholesterol is high and would you like a prescription for …?
But how do you know if you want a prescription for … or is there even another option?
So let’s start with what LDL and HDL actually are
Despite the names and associated reputation, LDL and HDL are not cholesterol.
They’re lipoproteins — tiny transport particles that carry cholesterol and fats through the bloodstream.
Cholesterol itself can’t travel freely in blood, it would need to be water-soluble to do that, so the body packages it into delivery vehicles.
Think of it like trucks on the motorway, – we absolutely need trucks to deliver all sorts of things to the right places, but get to many on the motor way and it gets clogged up!
(In the next episode of Nutrition Matters we go into greater detail about Cholesterol itself but for now lets just concentrate on these ‘trucks’).
LDL isn’t the villain — it’s the currier
LDL (low-density lipoprotein) delivers cholesterol from the liver to tissues that need it.
Your body requires cholesterol for:
- Hormone production (oestrogen, testosterone, cortisol)
- Cell membrane structure
- Brain and nerve function
- Vitamin D synthesis
So you see, LDL itself isn’t toxic. The problem begins when the system becomes overloaded or dysfunctional.
When there are too many LDL particles circulating, more cholesterol gets delivered than the tissues require. Excess particles begin to infiltrate artery walls.
This can happen because of:
- Genetics (familial hypercholesterolaemia)
- Diets that raise LDL in susceptible individuals (more about that next time)
- Insulin resistance
- Fatty liver
- Impaired LDL clearance
This build up triggers the immune system to send out special white blood cells called Macrophages that engulf the particles resulting the formation of ‘Foam cells’ which is how Plaque develops.
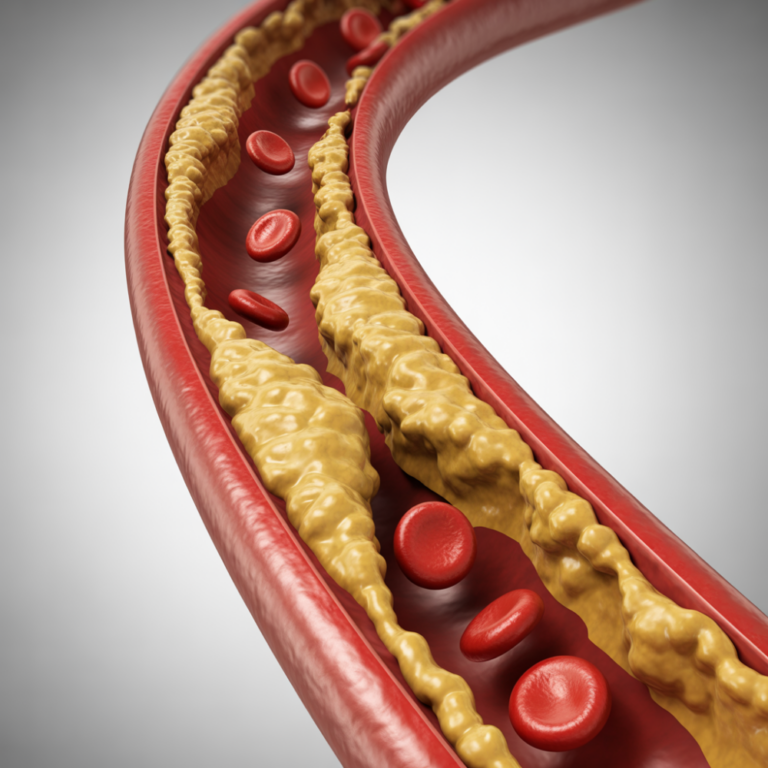
This is not simply a plumbing problem. It’s an inflammatory process.
Which brings us to ApoB
ApoB (Apolipoprotein B) -the shift most people haven’t heard about
In short, LDL isn’t the only particle that carries cholesterol it’s just the one we talk about most. But on each of these LDL-type particles there is exactly one ApoB molecule so by counting all the ApoB molecules you get to count all the cholesterol – carrying particles that matter for heart health.
In plain English:
ApoB tells you how many particles are circulating, which is what actually drives plaque formation. More particles = more chances to get stuck in artery walls – Cholesterol doesn’t clog arteries. Cholesterol‑carrying particles do.
LDLs become particularly dangerous inside an unhealthy metabolic environment.
Especially important for people with:
- Diabetes
- Insulin resistance
- Fatty liver
- Obesity
- Discordant lipid profiles (e.g., normal LDL-C but high particle numbers)
(Harvard Health)
And what about HDL — the “good” cholesterol?
HDL (high‑density lipoprotein) was long labelled protective. But the story is more nuanced. Because it’s HDL’s function that matters more than its quantity.
Its job is reverse cholesterol transport — collecting excess cholesterol and returning it to the liver. It also has anti‑inflammatory and repair roles.
But here’s the critical update:
When researchers tried raising HDL with medication, heart attack rates didn’t fall. That was the turning point. Higher HDL levels are associated with lower risk — but increasing HDL doesn’t reduce risk.
Which tells us something important.
- HDL reflects metabolic health.
- It doesn’t override LDL burden.
Even the best street sweepers cannot fix a city gridlocked with delivery trucks. HDL is a marker. LDL particle burden is a mechanism.
Where cardiometabolic science has landed
- LDL particle exposure over time drives atherosclerosis.
- ApoB gives a clearer picture of that particle burden.
- HDL level alone is not protective.
- Risk is cumulative — concentration × duration.
This isn’t hype. It isn’t trend‑based. It’s where decades of evidence have converged.
And no — I’m not a doctor. But anyone who took a BSc seriously learns how to read papers, not headlines. The goal here isn’t to prescribe. It’s to equip you.
Because informed decisions beat reactive ones every time.
The question that naturally follows
If LDL particle burden drives risk…
- Where do dietary fats fit into this picture?
- Do saturated fats raise particle number?
- Does carbohydrate quality matter?
- What about ultra‑processed food, insulin resistance, and metabolic context?
This is exactly where the debate gets noisy.
Subscribe to make sure you don’t miss the next three articles, where I’ll break down how dietary fats interact with LDL, ApoB, and metabolic health — without TikTok shortcuts, anti‑meat hysteria, or biohacker bravado. Just clear, evidence‑led guidance you can use immediately.
Because Real Nutrition Matters.
Niki Kerr is a qualified nutritionist, an award-winning writer and behaviour-change specialist. Bringing a thought-leader lens to Food, Nutrition and modern weight loss (including GLP-1 medications) with an evidenced focus on what actually works in real life: nourishment, consistency, and behaviour change that sticks.
Main References:
Feingold, K.R. and Grunfeld, C. (2000–2024). Introduction to Lipids and Lipoproteins. Endotext [Internet]. MDText.com, Inc.
National Lipid Association (2024). Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus. Journal of Clinical Lipidology, 18(5), e647–e663.
Scientific Advisory Committee on Nutrition (SACN) (2019). Saturated fats and health. Public Health England. Summary available via HEART UK – The Cholesterol Charity.
